In this article
- What Is the Difference Between CBT and DBT?
- The Quick Version
- How They Differ
- Philosophy
- Structure
- Skills Taught
- The Role of Acceptance
- Intensity of Treatment
- What Each Treats Best
- CBT Is Strongest For:
- DBT Is Strongest For:
- Both Work For:
- How to Decide
- They’re Not Mutually Exclusive
- What About DBT Skills Without Full DBT?
- A Note About the Therapeutic Relationship
- Making the Decision
- Frequently Asked Questions About CBT vs DBT
- Related Reading
Looking for a quick answer? See our DBT vs CBT comparison hub for a side-by-side at-a-glance and a 6-question decision aid. The article below is the deeper version.
What Is the Difference Between CBT and DBT?
CBT (Cognitive Behavioral Therapy) and DBT (Dialectical Behavior Therapy) are both evidence-based therapies under the cognitive-behavioral umbrella, but they are designed for different problems and work in fundamentally different ways. CBT focuses on identifying and changing distorted thought patterns that drive specific conditions like anxiety, depression, or OCD. DBT focuses on building skills to manage intense emotions, improve relationships, and tolerate distress — particularly for people whose emotional intensity makes standard CBT insufficient.
“Should I do DBT or CBT?” is one of the most common questions people ask when starting therapy. Here’s a clear, honest comparison to help you figure out which approach — or combination of approaches — fits your situation.
The Quick Version
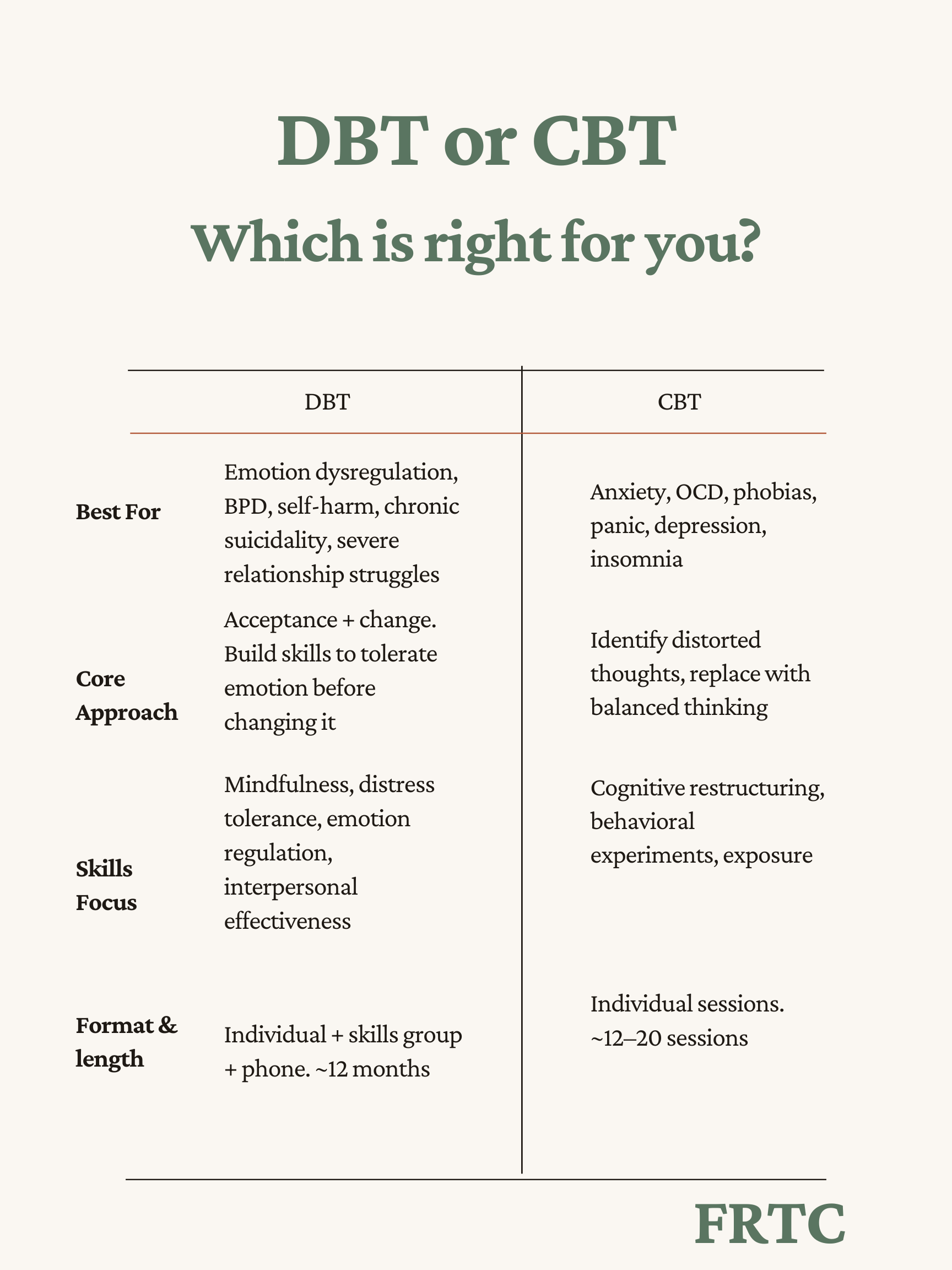
CBT is best when the primary problem is a specific, identifiable condition — anxiety, depression, OCD, phobias, insomnia — and the goal is to change the thought patterns and behaviors maintaining that condition.
DBT is best when the primary problem is emotional dysregulation — when emotions are consistently too intense, too reactive, or too slow to recover — especially when it affects relationships, impulse control, and overall functioning.
There’s significant overlap, and many people benefit from elements of both at different stages of treatment. But understanding the core difference between these two approaches helps you start in the right place and avoid wasting time on a treatment that doesn’t match your needs.
How They Differ
Philosophy
CBT operates on the premise that psychological suffering is largely driven by distorted thinking. If you change the thought, you change the emotion and the behavior. The therapy is focused on identifying cognitive distortions (catastrophizing, black-and-white thinking, mind reading) and replacing them with more accurate, balanced thoughts.
DBT starts from a different premise: that some people experience emotions so intensely that cognitive restructuring alone isn’t enough. Before you can change your thinking, you need to be able to tolerate the emotion that’s hijacking your thinking. DBT balances acceptance (radical acceptance, validation, mindfulness) with change (behavioral skills, problem-solving, exposure).
Structure
CBT is typically delivered in individual therapy sessions, usually 12-20 sessions for a specific condition. It’s focused, time-limited, and goal-oriented. You and your therapist work on a defined problem with measurable targets.
DBT is a comprehensive program with four components: individual therapy, skills training group, phone coaching, and consultation team. It typically lasts about 12 months. The structure is more intensive because it’s treating more pervasive patterns, not just a single condition.
Skills Taught
CBT teaches cognitive restructuring (identifying and challenging distorted thoughts), behavioral experiments (testing beliefs through action), exposure techniques, and problem-solving. The focus is on changing how you think about situations.
DBT teaches four categories of skills: mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness. The focus is on changing how you respond to emotions and navigate interpersonal relationships, while also learning to accept yourself as you are in this moment.
The Role of Acceptance
This is the biggest philosophical difference. CBT is primarily change-focused: the goal is to modify thoughts and behaviors that cause suffering. DBT holds change and acceptance as equally important — you work to change what you can while accepting what you can’t, and the dialectic between these two stances drives the therapy.
For some people, particularly those who’ve felt pushed to change without first feeling understood, DBT’s emphasis on validation and acceptance is what makes therapy feel safe enough to work. This is especially true for people who have spent years being told to “just think more positively” or “stop overreacting” — messages that, however well-intentioned, invalidate their experience and make change harder, not easier. DBT says: “Your feelings make sense given your experience, and there are skills that can help you respond to them more effectively.” Both parts of that statement matter.
Intensity of Treatment
CBT and DBT also differ in treatment intensity. CBT typically involves one session per week for a defined period — often 12 to 20 sessions. This makes it accessible, manageable, and well-suited for specific, circumscribed problems.
DBT asks for significantly more: weekly individual therapy, weekly skills group, phone coaching as needed, and daily homework practice. This level of commitment exists because the problems DBT treats are more pervasive and more deeply ingrained. Changing emotional patterns that have developed over a lifetime requires more sustained, intensive intervention than changing a specific cognitive distortion. The 4-miss rule in DBT reflects this philosophy — consistent attendance is not optional because the treatment builds on itself week to week.
What Each Treats Best
CBT Is Strongest For:
- Anxiety disorders (generalized anxiety, social anxiety, panic disorder)
- Depression (especially when driven by negative thought patterns)
- OCD (through Exposure and Response Prevention)
- PTSD (through Cognitive Processing Therapy or Prolonged Exposure)
- Specific phobias
- Insomnia
- Eating disorders (particularly bulimia and binge eating)
DBT Is Strongest For:
- Borderline Personality Disorder (the condition it was developed for)
- Chronic suicidality and self-harm
- Severe emotional dysregulation
- Impulsive or self-destructive behaviors
- Treatment-resistant depression (when standard approaches haven’t worked)
- Complex presentations where multiple issues co-occur
- Relationship difficulties rooted in emotional intensity
Both Work For:
- Depression (CBT through cognitive restructuring, DBT through behavioral activation and emotion regulation)
- Anxiety (CBT through exposure and thought challenging, DBT through distress tolerance and mindfulness)
- Trauma (CBT through PE/CPT, DBT through stabilization and skill-building)
- Interpersonal problems (CBT through assertiveness training, DBT through interpersonal effectiveness)
How to Decide
Ask yourself these questions:
Is my primary issue a specific condition (anxiety, OCD, depression) or a broader pattern of emotional instability? If specific → lean CBT. If broader → lean DBT.
Have I tried CBT or standard therapy before without lasting improvement? If yes → DBT may address what was missing.
Do my emotions frequently feel out of proportion to the situation? If yes → DBT’s focus on emotion regulation is specifically designed for this.
Am I dealing with self-harm, chronic suicidal thoughts, or severe impulsivity? If yes → DBT has the strongest evidence base for these issues.
Do I want focused, short-term treatment for a specific problem? If yes → CBT’s structure fits this goal.
Do I need help with relationships and emotional patterns, not just a single diagnosis? If yes → DBT’s comprehensive approach addresses the bigger picture.
They’re Not Mutually Exclusive
Many people benefit from both approaches at different points. Someone might start with DBT to build emotional stability and distress tolerance, then transition to CBT for targeted work on specific anxiety or trauma. Or someone might do CBT for depression and later add DBT skills training to address relationship patterns.
What About DBT Skills Without Full DBT?
An increasingly common middle ground is learning DBT skills without enrolling in a full comprehensive DBT program. Many therapists incorporate DBT skills — particularly mindfulness and emotion regulation — into CBT treatment. This can be effective for people whose primary issue responds well to CBT but who also benefit from DBT’s practical skills for managing emotional intensity.
However, for conditions where comprehensive DBT is the recommended treatment — particularly BPD, chronic suicidality, and severe emotional dysregulation — the full comprehensive model with all four components is what the research supports. Borrowing individual techniques from DBT while delivering a fundamentally different treatment is not the same as delivering DBT. If you’re unsure whether you need the full model or just some skills, a consultation with a DBT specialist can help clarify.
A Note About the Therapeutic Relationship
One aspect that both CBT and DBT share is the importance of the therapeutic relationship — but they approach it differently. In CBT, the relationship is collaborative and professional: you and your therapist work together as a team on defined problems. The relationship matters, but it’s primarily a vehicle for the work.
In DBT, the relationship is itself a therapeutic tool. Your DBT therapist uses the relationship to model effective interpersonal skills, provides validation that may counteract years of invalidation, and works through ruptures and repairs in the relationship as practice for interpersonal effectiveness. The phone coaching component means the relationship extends beyond the therapy hour into the moments where you need support most. For people whose core struggles are interpersonal, this relational intensity can be transformative.
Making the Decision
At Front Range Treatment Center, we offer both DBT and CBT, and our therapists help clients determine which approach — or combination — makes the most sense for their situation. The goal isn’t to fit you into a modality. It’s to find the treatment that fits your needs. During a free consultation, we can help you think through which approach aligns with what you’re experiencing and what you’re hoping to achieve.
Frequently Asked Questions About CBT vs DBT
Is DBT a type of CBT? Yes. DBT was originally developed by Marsha Linehan as a modification of CBT for people whose emotional intensity made standard CBT less effective. DBT retains CBT’s focus on changing unhelpful patterns but adds acceptance-based strategies, skills training, and a dialectical philosophy that balances change with validation.
Can you do CBT and DBT at the same time? Generally, clinicians recommend focusing on one at a time. If emotional dysregulation is severe, DBT typically comes first because it builds the emotional stability needed for CBT’s cognitive restructuring work. Many people start with DBT and transition to CBT for specific conditions (like OCD or phobias) once they have a foundation of emotional skills.
Which is better for anxiety — CBT or DBT? CBT has the stronger research base for specific anxiety disorders (social anxiety, OCD, phobias, panic disorder). However, if your anxiety is accompanied by emotional intensity that makes standard exposure work difficult, DBT’s distress tolerance and emotion regulation skills may be needed first. At FRTC we offer both CBT for anxiety and DBT-based anxiety treatment.
Related Reading
Looking for structured DBT?
FRTC programs related to this article.
Need Support?
Our team specializes in evidence-based DBT and CBT therapy. Reach out for a free consultation.